
 When we talk about what we need to do to make quality health care affordable and available to all, people (including card-carrying liberals like Barney Frank) tend to talk about the supposed need for medical malpractice reform, or about capping Medicare benefits or more comparative effectiveness research. But, in a nation where the top one percent earn twenty-four percent of the nation’s income and control forty percent of its wealth, no one seems to be talking about the effect that income inequality has on health care delivery and outcomes.
When we talk about what we need to do to make quality health care affordable and available to all, people (including card-carrying liberals like Barney Frank) tend to talk about the supposed need for medical malpractice reform, or about capping Medicare benefits or more comparative effectiveness research. But, in a nation where the top one percent earn twenty-four percent of the nation’s income and control forty percent of its wealth, no one seems to be talking about the effect that income inequality has on health care delivery and outcomes.
But that’s changing. Awhile back, I blogged about the new book “The Spirit Level,” about the negative effect that income inequality has on public health.
And recently a New Yorker article entitled “Poverty Clinic” drew more attention to cutting-edge research suggesting that poverty and trauma can, in and of themselves, cause poor health outcomes.
The new thinking traces its origins to a study commissioned by the Kaiser Permanente H.M.O. in the mid-1990s. The study measured patients’ so-called “Adverse Childhood Experiences” (ACE) scores and assessed the patients’ health. A lot of the circumstances that are factored into determining ACE score – such as growing up with parental divorce and family members with mental illness or substance dependency – also tend to disproportionately affect children living in poverty.
What the researchers found stunned even them.
Patients with high ACE scores grew up to be at very high risk for suicide, drug abuse, cancer and heart disease. The drug abuse and suicide didn’t surprise researchers that much. Initially researchers thought that the cancer and heart disease could easily be explained away too.
They hypothesized that the ACE scores/poverty of the patients was merely correlated with the heart disease and cancer and was not the cause of it. They imagined that poorer patients ate less healthy and their diet led to the cancer and heart disease problems.
But it turned out that it was more complicated than that. Researchers found that patients with high ACE scores who didn’t drink, who didn’t smoke and who were not overweight were three hundred percent more likely to suffer from heart disease. Childhoods filled with poverty and trauma were affecting patients’ health through some sort of causal mechanism that had nothing to do with unhealthy behaviors such as smoking or overeating.
The exact pathways by which childhood trauma lead to poor health are not well understood. But research shows that childhood adversity can actually alter the chemistry of DNA in the brain through a process called methylation. Childhood trauma can cause complex lifelong changes in endocrinology and brain chemistry.
As Dr. Vincent Felitti, one of the co-authors of the ACE study, points out, we spend billions of dollars each year on statins because we know that having a cholesterol reading above 240 doubles your chance of heart attack. But so does having an ACE score greater than 4.
So maybe, if we’re trying to reduce heart disease, we should be looking to reduce some of its root causes such as childhood poverty and its associated traumas.
Health care is not (solely) a budgetary issue. Addressing health care also means addressing other social issues, such as the poverty and inequality that many Americans are born into.
Category Archives: Medical Malpractice
The Two Ways Better Databases Would Drive Down Health Care Costs
 As we’ve blogged about a great deal here, the costs of medical malpractice don’t amount to a hill of a beans when we’re talking about the costs of health care generally. According to the journal Health Affairs, the direct costs of medical malpractice (insurance company payouts, payments to medical malpractice defense lawyers) and the indirect costs (the costs of so-called “defensive medicine”) amount to 2.4% of our nation’s annual health care tab.
As we’ve blogged about a great deal here, the costs of medical malpractice don’t amount to a hill of a beans when we’re talking about the costs of health care generally. According to the journal Health Affairs, the direct costs of medical malpractice (insurance company payouts, payments to medical malpractice defense lawyers) and the indirect costs (the costs of so-called “defensive medicine”) amount to 2.4% of our nation’s annual health care tab.
So while all the great new patient safety ideas that we blog about here – such as medical checklists and cockpit safety principles – hopefully catch on in medicine, they’re unlikely to change the curve of growing health care expenses.
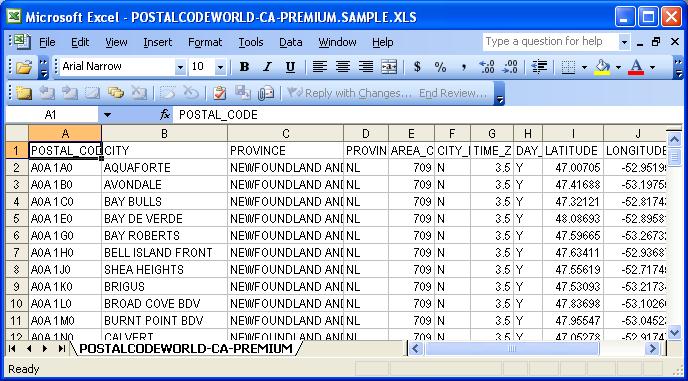
What could succeed in driving down health care costs is getting better databases to track health care spending. We already have databases with lots of health care spending data in them. What we need are smarter databases, databases that we can use to more easily manipulate the numbers and search for trends within them.
Smarter databases could help reduce health care spending in two ways. Smarter databases could reduce health care costs on the demand side by identifying patients who are costing us the most and targeting them for more efficient care. And smarter databases could reduce health care costs on the supply side by helping us identify unnecessary tests and procedures.
- The Demand Side –
Getting smarter databases will enable us to do the kind of “medical hot spotting” that promises to drive down health care costs. As we’ve previously blogged about, health care “hot spotting” is modeled after the Compstat crime-tracking system that many credit with contributing to the decline in crime rates that began in the 1990s. Just as Compstat uses crime data to micro-map police precincts and direct police resources to the areas where they are most needed, medical “hot spotting” uses health care data to identify the “high spending” patients. As one study in Camden, NJ demonstrated, thirty percent of the city’s health care spending was spent on one percent of the city’s residents. Identifying those high-cost patients helped the city get a handle on health care costs by targeting those high-cost patients for interventions – such as healthy cooking lessons and other social services – that, although pricey, resulted in a huge reduction in health care costs. Unfortunately, the nifty databases that allow researchers to ferret out high-cost patients for individual attention are not easy to come by. Companies like Verisk Analytics are spending millions developing proprietary algorithms to get the job done. Your run-of-the-mill databases can’t do hot spotting, but we could net a lot in savings if our databases could.
- The Supply Side –
As the journal Health Affairs has noted, the costs of medical malpractice are dwarfed by the costs of fee-for-service medicine. Because of fee-for-service we get doctors performing a lot of unnecessary tests and procedures. Eliminating those unnecessary tests and procedures would take a big chunk out of our health care costs.
How do we uncover which doctors are guilty of performing unnecessary tests and procedures? By combing through the data. That’s exactly what the Wall Street Journal is doing in its series “Secrets of the System” series – scrutinizing Medicare payment data and unveiling which doctors are performing unnecessary surgeries. Other databases, such as ProPublica’s “Dollars for Docs” database, enable us to connect up the kickbacks that some doctors receive from medical device manufacturers with the types of surgeries that they’re performing.
Medicare, insurance companies, and other entities already have all this information: it’s merely a matter of having the right software to ferret out the excesses.
We don’t need tort reform. We need smarter databases.
Hospital Disciplines Doctor Who Allegedly Performed Unnecessary Spinal Fusion Surgeries
 It was only a matter of time. With The Wall Street Journal uncovering eyebrow-raising increases in spinal fusion surgeries in its “Secrets of the System” series of investigative reports, and The New York Times running stories on back surgeons receiving kickbacks from medical device manufacturers, sooner or later an orthopedic surgeon was going to be disciplined as a result of malfeasance uncovered by great investigative journalism.
It was only a matter of time. With The Wall Street Journal uncovering eyebrow-raising increases in spinal fusion surgeries in its “Secrets of the System” series of investigative reports, and The New York Times running stories on back surgeons receiving kickbacks from medical device manufacturers, sooner or later an orthopedic surgeon was going to be disciplined as a result of malfeasance uncovered by great investigative journalism.
And it has apparently finally happened. The Wall Street Journal is reporting that Dr. Vishal James Makker, a Portland, OR-based neurosurgeon has had his admitting privileges suspended by the hospital he worked at after the Journal ran a March 29 story showing that Dr. Makker performed ten times as many spinal fusion surgeries as the national average. According to the WSJ, in 2006 the Oregon board of medicine ordered Dr. Makker to undergo remedial training for what it called “unnecessary surgeries.”
(All of which makes you wonder, if Dr. Makker was a guy who the board of medicine five years ago determined was performing unnecessary surgeries, why is he still licensed to practice?).
Dr. Makker’s case is just a single illustration of a larger back-and-forth in the medical malpractice debate. Tort reformers claim that medical malpractice lawsuits drive up health care costs by encouraging doctors to practice “defensive medicine” – ordering unnecessary tests and procedures merely to provide cover in the event of a lawsuit. Patient advocates, citing a growing body of data, say that the performance of unnecessary tests and procedures is driven by the financial incentives doctors face in a world of fee-for-service medicine: more tests and procedures mean more money for doctors and their hospitals. Many doctors, whether consciously or unconsciously, are responding to those incentives.
We need to rearrange those incentives. We need to reward doctors financially for preventative care and the money they save and stop paying them for each cutting-edge procedure that they perform.
When we have a system that enriches people like Dr. Makker, we should not be surprised that there are Dr. Makkers out there.
The New Social Science Of Group IQ And How It Applies In The Operating Room
 David Brooks, The New York Times columnist, recently revived his blog, which you can find here. It’s a great aggregator of new results in cognitive psychology. Anyway, in poring through some of his older posts, I came across this discussion of the concept of group IQ. It’s a concept that’s been around for some time, but that has special application to medical malpractice that I don’t recall seeing anything about.
David Brooks, The New York Times columnist, recently revived his blog, which you can find here. It’s a great aggregator of new results in cognitive psychology. Anyway, in poring through some of his older posts, I came across this discussion of the concept of group IQ. It’s a concept that’s been around for some time, but that has special application to medical malpractice that I don’t recall seeing anything about.
“Group IQ” refers to the collective IQ of a group of people working together as a team, collaborating on some project (say, a medical operation). What is the measure of a group’s IQ? It might be natural to think that a group’s IQ is simply the average of its individual members’ IQs. You might think that if you have a really smart person in a group or a lot of smart people in a group that the group’s overall IQ would be really high as well.
But the research shows that this rather natural assumption does not hold. Instead, lots of groups show IQ that is much greater than the sum of its team members’ intelligences. There’s a certain gestalt effect within some groups where a collection of average individual intelligences become super-charged and work together astonishingly effectively as a group, enabling them to best a team of Einsteins.
The research shows that the team members of these overachieving groups share certain traits. The team members of groups with high group IQs are good at reading each other’s emotions. They take turns when speaking. Conversation in their groups tends to be widely distributed. There is no overbearing leader dominating everything.
It seems to me that operating rooms are run exactly opposite to what we now know about group IQ. Operating rooms are an example of the old myths about group intelligence: that you let your individual superstar (say a high-IQ surgeon) run the show and get out of his way, instead of looking for ways for everyone to participate. I recently blogged about Dr. James Bagian’s new article on patient safety. In the article, Bagian talks about how operating room culture is a “hero” culture, with the notion being that the surgeon is the hero and that others in the operating room – nurses, anesthetists, medical residents – are his inferiors.
That’s why we shouldn’t be astonished when brilliant surgeons make mind-numbing mistakes (see here). It’s simply the inevitable result of the group dynamics of the operating room, where a nurse does not feel empowered to question a doctor.
A lot of the aviation safety principles that Dr. Bagian urges medicine to adopt are principles that agree with what we know about group IQ. For example, airlines have a “first name rule” – airline crew call each other by their first names so that everyone’s on an equal rank and the captain isn’t some imperious demigod. You can see how this would reinforce some of the traits that high IQ groups have, such as widely distributed conversation and listening.
Reducing medical malpractice doesn’t turn on getting smarter doctors or better technology. It turns on adopting the methods that we know crank up a group’s performance.
Applying The Lessons Of Flight Safety To Medical Malpractice
 It’s a subject that we’ve blogged about a lot: how applying aviation safety principles to medicine could revolutionize the practice of medicine and reduce the incidence of medical malpractice. (See earlier blog posts here and here).
It’s a subject that we’ve blogged about a lot: how applying aviation safety principles to medicine could revolutionize the practice of medicine and reduce the incidence of medical malpractice. (See earlier blog posts here and here).
Now Dr. James Bagian (whom we’ve previously blogged about here), a doctor and pilot, has co-authored a journal article about the specific lessons that medicine should be learning from aviation. You can read the article for yourself here. (H/t WSJ Health Blog). Unlike a lot of peer-reviewed journal articles, it’s on a level that’s completely accessible to the layperson. I hope to be able to comment on the article more extensively in the near future.
Supervisors Of Medical Residents Don’t Think Cutting Residents’ Hours Will Reduce Residents’ Fatigue
 According to a recent study by the Accreditation Council for Graduate Medical Education, nearly two-thirds of the physicians who supervise medical residents doubt that a new regulation capping residents’ workdays at sixteen hours will reduce residents’ fatigue. (H/t WSJ Health Blog).
According to a recent study by the Accreditation Council for Graduate Medical Education, nearly two-thirds of the physicians who supervise medical residents doubt that a new regulation capping residents’ workdays at sixteen hours will reduce residents’ fatigue. (H/t WSJ Health Blog).
According to one of the doctors responsible for this survey, the survey’s respondents might doubt the effectiveness of cutting hours in reducing fatigue for a couple of reasons. First, the residents might not be less fatigued because they might use their time off to do something other than sleep. Second, residents who work fewer hours might rush more to cram all their work into a shorter day, leaving them more frazzled.
Overall, I think the medical profession is simply in denial about the issue of physician fatigue. As I blogged about a few weeks ago, a new study published in the Journal of the American College of Radiology shows that physician fatigue shows that fatigue sets in even over the course of an eight-hour (8:00 a.m.-4:00 p.m.) workday. By the end of an eight-hour shift, radiologists were twice as likely to make mistakes in reading a simple x-ray.
Doctors always protest that long hours are necessary for residents to learn all that they need to know. But residents are cash cows for teaching hospitals – their low salaries and the high-level tasks that they perform are very lucrative for hospitals. Reducing residents’ hours means that hospitals have to do more of their staffing with more senior doctors, whose salaries are much higher.
It’s time for medicine to come to grips with the problem of physician fatigue.
Look How Easy It Is To Reduce Medical Malpractice: New York Patient Safety Program Reduces Birth Injuries By 99 Percent (!!!)
 File it under news that no one is talking about but that everyone should be: a new study published in the American Journal of Obstetrics and Gynecology reveals that a new obstetric safety program implemented in several New York hospitals has reduced medical malpractice payouts in those hospitals by 99 percent!
File it under news that no one is talking about but that everyone should be: a new study published in the American Journal of Obstetrics and Gynecology reveals that a new obstetric safety program implemented in several New York hospitals has reduced medical malpractice payouts in those hospitals by 99 percent!
That number is so large that it almost takes a minute for it to sink in. A 99 percent reduction in medical malpractice payouts. One more percentage point and there would have been a one hundred percent reduction in medical malpractice payouts, meaning that medical malpractice would have cost insurers absolutely nothing! Zero dollars and zero cents. And all of this was accomplished in the span of three years with the implementation of this new safety program.
Of course medical malpractice payouts are not really a good surrogate for patient safety; payouts might go down because the hospitals got better defense lawyers. Or because injured patients can’t find plaintiffs’ lawyers willing to take their cases.
But the study also suggests that patient safety improved just as much as the hospitals’ bottom lines. So-called “sentinel events” — avoidable deaths and serious injuries — zeroed out during the course of the study.
What were the magical elements in this obstetrics safety program that proved so shockingly effective at preventing birth injuries? Was it a bunch of new, costly high-tech gizmos?
Although the hospitals that participated in the study abandoned their whiteboards in favor of a new system of electronic communications, a lot of the program’s features were decidedly low-tech and addressed a lot of the basic reasons why doctors make mistakes.
For instance, the participating hospitals each added three more physician assistants to their staffs and a “laborist” (a new term for an OB-GYN who works full-time for a hospital, much like a “hospitalist” in internal medicine). These additional staff members helped reduce physician fatigue, a major cause of medical malpractice that we’ve blogged about a great deal, most recently here.
Another low-tech safety innovation was the hiring of a full-time patient safety nurse who was responsible for educating staff on patient safety and conducting emergency drills.
These additional staff members and the new computers cost money. Do you think that if damages for pain-and-suffering in a birth injury case, such as a cerebral palsy case, were capped at $250,000 that hospitals would bother investing in these new safety measures? Where would their incentive be?
Medical malpractice can be easily reduced. That we might see medical malpractice in one sector almost completely eliminated over the course of a few years is, however, something of great surprise and a great cause for hope.
You can read more about the study here: “Obstetricians take big steps to avoid malpractice” (Crain’s New York Business.com).
CDC Reports That Number Of Central-Line Infections In Hospitals Is Dropping (We Can Do A Lot Better Though)
 According to the Centers For Disease Control, the number of central line infections in hospital ICUs has dropped fifty-eight percent since 2001. A central line infection might not seem like a big deal, but they are extremely serious: between twelve and twenty-five percent of patients who contract a central line infection die as a result. These deaths are part of the 98,000 deaths that are caused annually by preventable medical errors.
According to the Centers For Disease Control, the number of central line infections in hospital ICUs has dropped fifty-eight percent since 2001. A central line infection might not seem like a big deal, but they are extremely serious: between twelve and twenty-five percent of patients who contract a central line infection die as a result. These deaths are part of the 98,000 deaths that are caused annually by preventable medical errors.
But really there’s no reason why we can’t get the number of central line infections to zero, or some asymptotically low level.
As I’ve previously blogged about, virtually all central line infections could be eliminated if doctors and nurses followed the simple five-step procedure for properly inserting a central line. However, at least one-third of the time, medical staff skip at least one of the steps, putting the patient at risk for infection.
Insertion of central lines is one area where hospitals could definitely benefit from rigid adherence to medical checklists. As we’ve often blogged about, a World Health Organization study shows that the use of medical checklists can reduce surgical deaths by forty-seven percent and major complications by thirty-six percent. Yet most American hospitals still don’t require the use of checklists.
Young Doctors’ Overreliance On CT Scans
 In a New York Times op-ed piece published last week, entitled “Treat the Patient, Not the CT Scan,” Dr. Abraham Verghese takes young doctors to task for their overreliance on sophisticated medical imaging procedures, such as CT scans.
In a New York Times op-ed piece published last week, entitled “Treat the Patient, Not the CT Scan,” Dr. Abraham Verghese takes young doctors to task for their overreliance on sophisticated medical imaging procedures, such as CT scans.
Dr. Verghese hits on some points about the use of CT scans that are familiar to readers of this blog – the extremely high amounts of radiation that patients are exposed to by medical imaging (it now accounts for more than 50 percent of the radiation that Americans are exposed to) and the high price tag of such procedures (a huge driver of our health care costs, given how much cutting-edge medical imaging is overused).
But Dr. Verghese really hones in a point that would have Drs. Jesse Pines and Zachary Meisel (figures whom we’ve previously blogged about here) nodding in agreement: the overuse of medical imaging is both a cause of, and effect of, a deterioration in young doctors’ basic clinical skills.
Dr. Verghese relates the story of a woman who was admitted to the Emergency Room with seizures and breathing difficulties. Doctors instantly ordered a CT scan of her chest. It revealed she had massive breast tumors and the breast cancer had spread and caused secondary cancers.
Although the CT scan detected the cancer, Dr. Verghese believes that the overuse of CT scans may have led to its becoming so advanced without any medical intervention. Dr. Verghese writes:
In retrospect, though, her cancer should have been discovered long before the radiologist found it; before the emergency, the patient had been seen several times and at different places, for symptoms that were probably related to the cancer. I got to see the CT scan: the tumor masses in each breast were likely visible to the naked eye — and certainly to the hand. Yet they had never been noted.
Maybe instead of a conversation about capping damages in medical malpractice cases, we should be having a conversation about our overreliance on medical imaging, the massive amounts of radiation we are absorbing as a result of that overreliance and the cost of that overreliance – both in terms of health care quality and in dollars.
What Kind Of Conservative Believes In Tort Reform?
 Law professor William Jacobson senses a tension, bordering on self-contradiction, in two ideas favored by conservatives: the repeal of the Affordable Care Act (what is often styled as “Obamacare”) and support for tort reform measures, such as H.R. 5, a bill that I’ve previously blogged about, that would cap, by federal law, the damages that can be awarded in medical malpractice lawsuits filed in state court and litigated under state medical malpractice laws. (H/t Volokh Conspiracy).
Law professor William Jacobson senses a tension, bordering on self-contradiction, in two ideas favored by conservatives: the repeal of the Affordable Care Act (what is often styled as “Obamacare”) and support for tort reform measures, such as H.R. 5, a bill that I’ve previously blogged about, that would cap, by federal law, the damages that can be awarded in medical malpractice lawsuits filed in state court and litigated under state medical malpractice laws. (H/t Volokh Conspiracy).
Wherein lies the contradiction? Well, conservatives are normally backers of states rights. They like to trumpet the Tenth Amendment, which says, “The powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.”
Thus, they oppose the Affordable Care Act on the grounds that it exceeds the federal government’s powers to enact an individual health care mandate. They would have no constitutional objection to a state government enacting an identical mandate, but they believe that, under the Constitution, an individual mandate exceeds the federal government’s limited powers.
Lo and behold, when it comes to tort reform, conservatives’ qualms about the federal government’s powers vanish. There they favor the federal government intruding upon the administration of state medical malpractice law in state courts. Carrying the torch of tort reform, these same conservatives favor the imposition of a federal law capping pain-and-suffering damages in medical malpractice cases at a quarter of a million dollars.
They believe that Congress has the authority to pass such a law pursuant to its Commerce Clause powers; the same powers that they also say are not substantial enough to undergird the Affordable Care Act.
For consistency’s sake, congressional Republicans should jettison either their opposition to the Affordable Care Act or their support for capping damages in medical malpractice cases.