
 The headlines are hard to reconcile. This week, the journal Health Affairs published an article showing that American doctors are paid more per service – in some cases double! – than any of their foreign counterparts. American primary care physicians are paid approximately seventy percent more per office visit than doctors in other developed countries. And American specialists rake in even more: US orthopedic surgeons earn approximately 120 percent more for a hip replacement than surgeons in other countries. The study went on to find that these higher fees earned by American doctors are not connected to higher practice costs (such as malpractice premiums, rent, office staff salary). It’s no wonder that our doctors are, far and away, the world’s best paid.
The headlines are hard to reconcile. This week, the journal Health Affairs published an article showing that American doctors are paid more per service – in some cases double! – than any of their foreign counterparts. American primary care physicians are paid approximately seventy percent more per office visit than doctors in other developed countries. And American specialists rake in even more: US orthopedic surgeons earn approximately 120 percent more for a hip replacement than surgeons in other countries. The study went on to find that these higher fees earned by American doctors are not connected to higher practice costs (such as malpractice premiums, rent, office staff salary). It’s no wonder that our doctors are, far and away, the world’s best paid.
Yet a week earlier, the Mayo Clinic published a study finding widespread burnout among young physicians.
How is it that doctors are both handsomely paid and burned out on their profession?
I think the answer ties into some of my recent posts on abolishing licensure requirements for lawyers.
The medical and legal professions’ regulation of their members is a carryover of the medieval guild system in which artisans were required to be guild members in order to ply their trade. The guild system operated primarily for the benefit of those at the top of the profession – the master craftsmen. The others involved in the guild system – apprentices and journeymen – worked long and hard to pay their dues.
Medicine is the same way. Young residents work 100 hour weeks to pay their dues and work their way up. Doctors in the early stages of their careers work long hours to build up practices on their own, or to cover for older doctors if they are part of a group practice. Finally, in the last leg of their careers, many older doctors simply kick back and cash their large paychecks.
And those large paychecks are possible only when a guild system artificially constricts entry into the medical profession. The fact that many young doctors are concluding that the rat race is not worth it and that we have a looming shortage of primary care physicians suggests that the guild system is broken in medicine. The solution – one which would lower our health care costs as well as improve the happiness of medical professionals – is to let medicine be practiced by more than those who went to medical school.
Category Archives: Medical Malpractice
We Spend The Most On Health Care And Have The Least To Show For It In Terms Of Patient Safety
 It’s a familiar theme: Americans spend the most on health care, and often get the least in return. Last December, I blogged about how we spend the most per patient on dialysis treatment and have the world’s highest dialysis mortality rate.
It’s a familiar theme: Americans spend the most on health care, and often get the least in return. Last December, I blogged about how we spend the most per patient on dialysis treatment and have the world’s highest dialysis mortality rate.
Now, from medicalcodingandbillingcertification.net, comes a new infograph that sets out how our hospitals are among the world’s most unsafe, despite our spending the most on health care. (H/t Andrew Sullivan). The infograph breaks down the reason why US hospitals rank last out of 19 developed countries in preventable hospital deaths.
You stand a 1 in 300 chance of dying in an American hospital due to medical error. (By way of contrast, the average American stands a 1 in 10,000,000 chance of dying in a plane crash).
In American hospitals, 1 in 7 hospital-acquired infections lead to death, while in Europe only 1 in 122 do so. 99,000 people die due to hospital-acquired infections in the US each year. American doctors only wash their hands about one-quarter of the number of times that they should.
The long hours of medical residents are another reason why American hospitals lag in safety. Residents who work five or more 24 hour shifts in a month are seven times as likely to make a medical error as their peers. Also, doctors leaving the hospital after a 24-hour shift are 168% more likely to be in a car accident on their way home.
Sometimes you get what you pay for. In American health care, we don’t.
A New “Hotspot” Video
We’ve blogged before about so-called “medical hot spotting.” The technique promises to bring down the costs of health care dramatically by concentrating health care resources in the right places, much like, in the mid-1990s, police began to bring down crime rates by concentrating police patrols in the right areas. Now PBS’ Frontline has done a ten minute segment on hot spotting, which you can watch here:
Link Roundup
- Hundreds of doctors who have been disciplined by their own hospitals or insurance companies have escaped discipline by the board of medicine in California, according to this Los Angeles Times expose. The personnel at the board of medicine blame budget cuts for their inability to keep up with doctor misconduct.
- The Freakonomics blog features a new research study showing that a car that weighs 1,000 pounds more than the average car is forty-seven more percent likely to cause a fatality when it is involved in an accident with another car.
- The New York Times Magazine publishes an article by Dr. Darshak Sangavi entitled, “The Phantom Menace of Sleep-Deprived Doctors.” (I hope to be able to blog a response to this article in the near future).
Kaiser Health Sues Hospital Chain For Padding Bills
 Kaiser Health, one of the largest health insurance companies in the nation, is suing Prime Health Services, Inc., for taking Emergency Room patients and unnecessarily having them stay for extended periods of times on an in-patient basis, as part of an alleged scheme to drive up the price tag of the hospital visits.
Kaiser Health, one of the largest health insurance companies in the nation, is suing Prime Health Services, Inc., for taking Emergency Room patients and unnecessarily having them stay for extended periods of times on an in-patient basis, as part of an alleged scheme to drive up the price tag of the hospital visits.
Patients who were victimized by this practice report having difficulty checking themselves out of the hospital — even when they were in good health.
This is just another example of the biggest problem with American health care. The costs of medical malpractice — direct and indirect — are a tiny portion of health care spending. The real problem with American health care is that the financial incentives all align for providing unnecessary care and overtreating, rather than preventative care.
When Doctors Follow Evidence-Based Guidelines Only 54 Percent Of The Time, You Get A Lot Of Unnecessary Surgeries
 In 2003, Dr. Elizabeth McGlynn and her coauthors published a blockbuster study in The New England Journal of Medicine showing that American doctors follow evidence-based guidelines only 54 percent of the time, meaning that when you receive medical treatment there’s a 50/50 chance that the treatment you’re receiving has no scientific validity to it.
In 2003, Dr. Elizabeth McGlynn and her coauthors published a blockbuster study in The New England Journal of Medicine showing that American doctors follow evidence-based guidelines only 54 percent of the time, meaning that when you receive medical treatment there’s a 50/50 chance that the treatment you’re receiving has no scientific validity to it.
The tendency within American medicine to recommend surgeries and other procedures that are not backed by evidence-based practices leads to a lot of unnecessary incisions and health care costs. Nearly two months ago, I blogged about how a large number of stent surgeries are performed in circumstances outside of those recommended by the guidelines.
Now comes new research, published in the Journal of the American Medical Association, showing that twelve percent of balloon angioplasties are performed on patients under circumstances where evidence-based guidelines do not recommend it. In some hospitals, as many as twenty percent of the balloon angioplasties that were performed were outside of the guidelines.
Tort Reform And Health Care Cost Control
Via Andrew Sullivan, a very interesting pie chart:
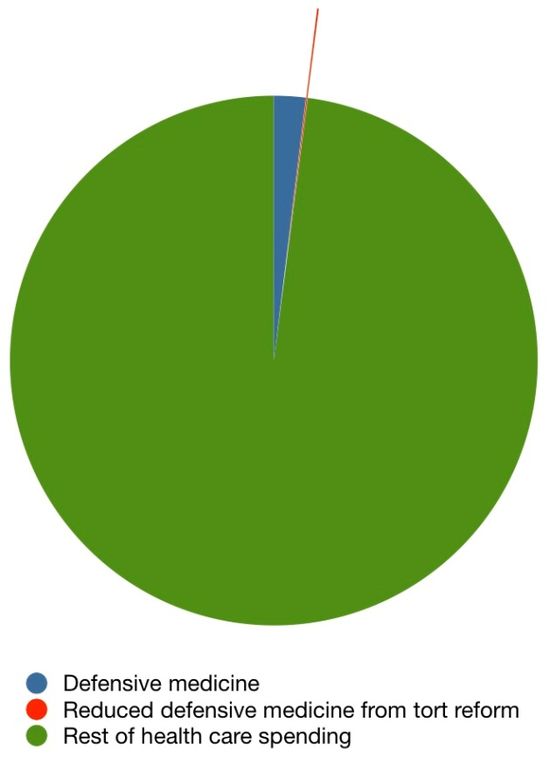
It’s from research by economist Aaron Caroll, showing that states that have enacted caps on damages in medical malpractice cases haven’t reaped savings.
This shouldn’t come as any surprise given that all of the costs associated with medical malpractice – from medical bills for the injured to lawyer fees – only add up to 0.5% of our health care spending.
Cutting down on payouts in medical malpractice cases won’t bring down our health care costs. They’ll only guarantee that the taxpayer foots the bill for the injuries, rather than the medical malpractice insurer.
Forty Years And Medicine Still Has Not Changed
 Today’s Los Angeles Times carries an op-ed co-authored by Dr. Lucian Leape of Harvard’s School of Public Health on the topic of resident fatigue.
Today’s Los Angeles Times carries an op-ed co-authored by Dr. Lucian Leape of Harvard’s School of Public Health on the topic of resident fatigue.
July marks the month that young doctors begin their residencies at teaching hospitals across the country.
This month also marks the fortieth anniversary of a landmark article published in The New England Journal of Medicine that showed for the first time how much fatigue affects a doctor’s performance. The landmark article showed that sleep-deprived residents made twice as many errors reading electrocardiograms as well-rested residents.
Yet despite being aware, for nearly half a century now, that sleep-deprived residents were endangering patients, the medical community has done very little to remedy the problem.
In recent years, first-year residents have had their shifts capped at sixteen hours – a step in accordance with sleep science. But hospitals can force second- and third-year residents to work shifts of up to twenty-eight hours with little or no sleep.
Such policies are contrary to sleep science research, which demonstrates that human performance falls off a cliff after about sixteen hours of wakefulness.
Teaching hospitals, however, continue to have residents work long hours because the low-salaried residents are lucrative cash cows for the hospitals.
For more on this issue, check out last July’s blog post on the “July Effect.”
New Report Estimates Wrong Site Surgeries Take Place 40 Times Each Week
 As reported by The Washington Post, a new report by a hospital accreditation body estimates that so-called wrong site surgeries take place 40 times each week in the nation’s hospitals.
As reported by The Washington Post, a new report by a hospital accreditation body estimates that so-called wrong site surgeries take place 40 times each week in the nation’s hospitals.
Wrong site surgeries are operations that take place on the wrong part of the body, such as amputations of healthy limbs, back surgeries that are performed on the wrong vertebrae, etc.
Wrong site surgeries are so common in fact that one in four orthopedic surgeons will make a wrong site error in their careers, according to the American Academy of Orthopaedic Surgeons.
The tragedy is that wrong site surgeries are among the most preventable kind of medical malpractice. Pre-surgery “timeouts” where the surgical team reviews the surgery, including surgical site, have been shown to dramatically reduce the incidence of wrong site surgery. In seventy-two percent of wrong site surgeries, the surgical team was found not to have stopped for a timeout.
And yet surgeons are resistant to adopting universal timeouts.
Perhaps surprising to a lot of tort reformers, only one-third of wrong site surgeries result in a medical malpractice claim. In fact, the wrong site involving Dr. Peter Ring of Boston (which we blogged about last year) never resulted in a medical malpractice lawsuit being filed, perhaps because of the conspicuous bravery and honesty of Dr. Ring, who bucked the medical system’s code of silence and used his wrong site surgery as a teachable moment.
As commendable as Dr. Ring’s conduct was, however, we need more than surgeons who are humble enough to publicly acknowledge their errors. We need surgeons who are willing to adopt the proven tactics – such as surgical timeouts and checklists – that can help eradicate wrong site surgeries.
Massachusetts Considers Law Giving Patients The Right To Have Their Surgery Videotaped
 The Massachusetts legislature is weighing a bill that would give patients the right to have their surgery videotaped if they paid for the recording. Hospitals that refused to allow videotaping would face a $10,000 fine.
The Massachusetts legislature is weighing a bill that would give patients the right to have their surgery videotaped if they paid for the recording. Hospitals that refused to allow videotaping would face a $10,000 fine.
The bill had a hearing Tuesday before the Public Health Commission.
Personally, I think that in many surgeries the videos would be of little value in proving medical malpractice because so much of surgery requires working in tight confines that cameras can’t peer into.
But the psychological effect of recording may prompt surgeons to be more attentive and courteous, thus contributing to patient safety.